


Cognitive Functioning in Addiction and Recovery
Cognitive Functioning in Addiction
and Recovery
By Dr. Terry Spokes, DClinPsych

Dr. Terry Spokes, DClinPsych (University of Oxford)
Dr. Spokes has led residential treatment programmes across multiple centres and clinical settings. At The Winslow, he oversees clinical care and programming, delivering personalised, evidence-based treatment for sustained recovery.
When attempting to understand addiction, it is essential to adopt a multi-faceted lens. Addiction impacts multiple domains of an individual’s life – biological, psychological, social, and behavioural – and rarely presents in the same way for any two people. Each person brings a unique constellation of experiences, beliefs, patterns, and ways of making meaning that shape what resonates and what supports change.
It is therefore important to explore how addiction manifests across different areas of an individual’s life. This may include its impact on physical health, relationships, emotional and psychological wellbeing, sense of meaning or spirituality, and day-to-day functioning, such as work or study. It is equally important to understand a person’s level of insight, their current understanding of addiction, and their readiness to engage in change.
One area that often receives less attention is cognitive functioning. This refers to thinking processes such as attention, memory, and planning. Within this, executive functioning is particularly important – it underpins decision-making, behavioural regulation, and problem-solving. A growing body of research shows that addiction is associated with impairments in executive functioning, particularly in inhibitory control, working memory, and decision-making. These difficulties are clinically meaningful, as they are linked to poorer treatment engagement and a higher risk of relapse.
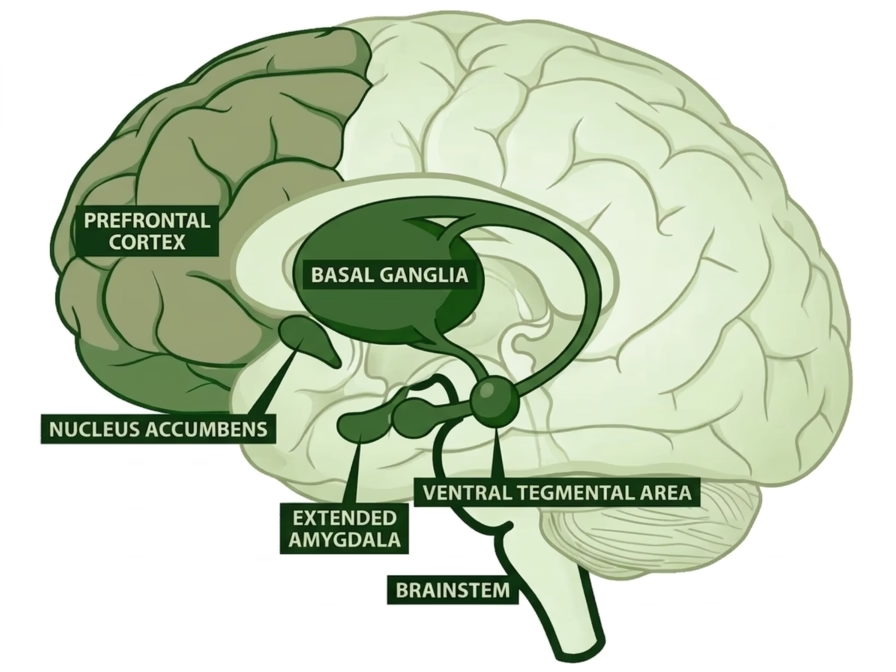
Source: Addiction Center https://www.addictioncenter.com/addiction/brain/
Cognitive functioning is closely linked to underlying brain systems. Impairments in executive functioning seen in addiction have been associated with changes in dopaminergic and glutamatergic activity across cortical and midbrain regions. These changes help explain why individuals may struggle with impulse control, planning, and adapting behaviour, even when they are motivated to change. Importantly, similar patterns have been observed in both substance-related and behavioural addictions.
Many treatment approaches focus on strengthening conscious decision-making, for example, by helping individuals identify high-risk situations to avoid and supportive environments to engage with. While valuable, this alone is often insufficient.
Relapse in early recovery is frequently less about a lack of knowledge and more about a reduced capacity to inhibit automatic responses, regulate attention, manage emotional discomfort, and plan ahead. These processes are shaped by neural systems operating outside of conscious awareness and may take time to recover.
For this reason, treatment should also incorporate approaches that support neurocognitive recovery – targeting areas such as attention, inhibitory control, and cognitive flexibility. Strengthening these capacities, through interventions such as repetitive transcranial magnetic stimulation (rTMS), attention training, or cognitive rehabilitation, can enhance self-regulation, reduce impulsivity, and support individuals to navigate high-risk situations more effectively.
In doing so, we can help build greater resilience against relapse and support more sustainable, long-term recovery.

Transcranial Magnetic Stimulation in Addiction Treatment
Transcranial Magnetic Stimulation in Addiction Treatment: A Consultant Addiction Psychiatrist’s Perspective
By Dr. Sharad Haridas, MBBS, MRCPsych (London), FAMS (Psych)

Dr. Sharad Haridas, MBBS, MRCPsych (London), FAMS (Psych)
Dr. Haridas is a dual-registered consultant psychiatrist and addiction specialist with 16 years of experience in London. At the Winslow, he oversees TMS for clients with addiction using evidence-based, personalised treatment pathways. He is a Fellow of the Clinical TMS society (International).
For those working at the intersection of addiction psychiatry and neuromodulation, it is both an exciting and a cautiously optimistic time. Transcranial magnetic stimulation (TMS) has been a tool in the psychiatric armamentarium for four decades now, since Professor Anthony Barker and his team at the University of Sheffield demonstrated the first functional TMS device in 1985. In that time, the technology has matured from a laboratory curiosity into a clinically validated treatment for depression, obsessive-compulsive disorder, migraine, and most recently, smoking cessation. Its application to substance use disorders is still developing. It shows real promise, but research methods and heterogeneity vary widely, and institutions seem to be rightly but excessively cautious about adopting it as a standard treatment.
This article is not intended as an exhaustive systematic review. Rather, it reflects the perspective of a clinician who has been delivering TMS in the context of addiction treatment for a number of years, and who wishes to share a practical, evidence-informed account of where TMS fits — and where it does not — in the treatment of substance use disorders.
A Primer on the Mechanism
For colleagues less familiar with TMS, the basic mechanism is worth revisiting. A figure-of-eight coil is placed against the scalp. An electrical current passes through the coil, which in turn generates a focused magnetic field that passes through the skull without impedance. This then induces a local electrical current in the underlying cortical tissue causing depolarisation. Unlike electroconvulsive therapy (ECT), which delivers electrical current directly to the scalp to induce a generalised seizure, TMS is typically administered at subthreshold levels for seizure induction while remaining above the threshold for local depolarization. The individual remains fully conscious throughout, experiences no anaesthesia, and can typically resume normal activities immediately after treatment.
The most common target in both depression and addiction protocols is the left dorsolateral prefrontal cortex (DLPFC), a region central to executive function, impulse control, and top-down regulation of deeper limbic and reward-related brain structures. In addiction, there is compelling evidence that the prefrontal cortex is functionally underactive, particularly in alcohol and stimulant use disorders, while subcortical structures — the amygdala, insula, and ventral striatum — tend toward overactivation. This mismatch between cortical control and subcortical drive is a hallmark of the addicted brain, and it maps closely onto what is observed in addiction or any compulsive use behaviours: diminished impulse control, heightened cue reactivity, and difficulty maintaining behavioural change despite sincere motivation.
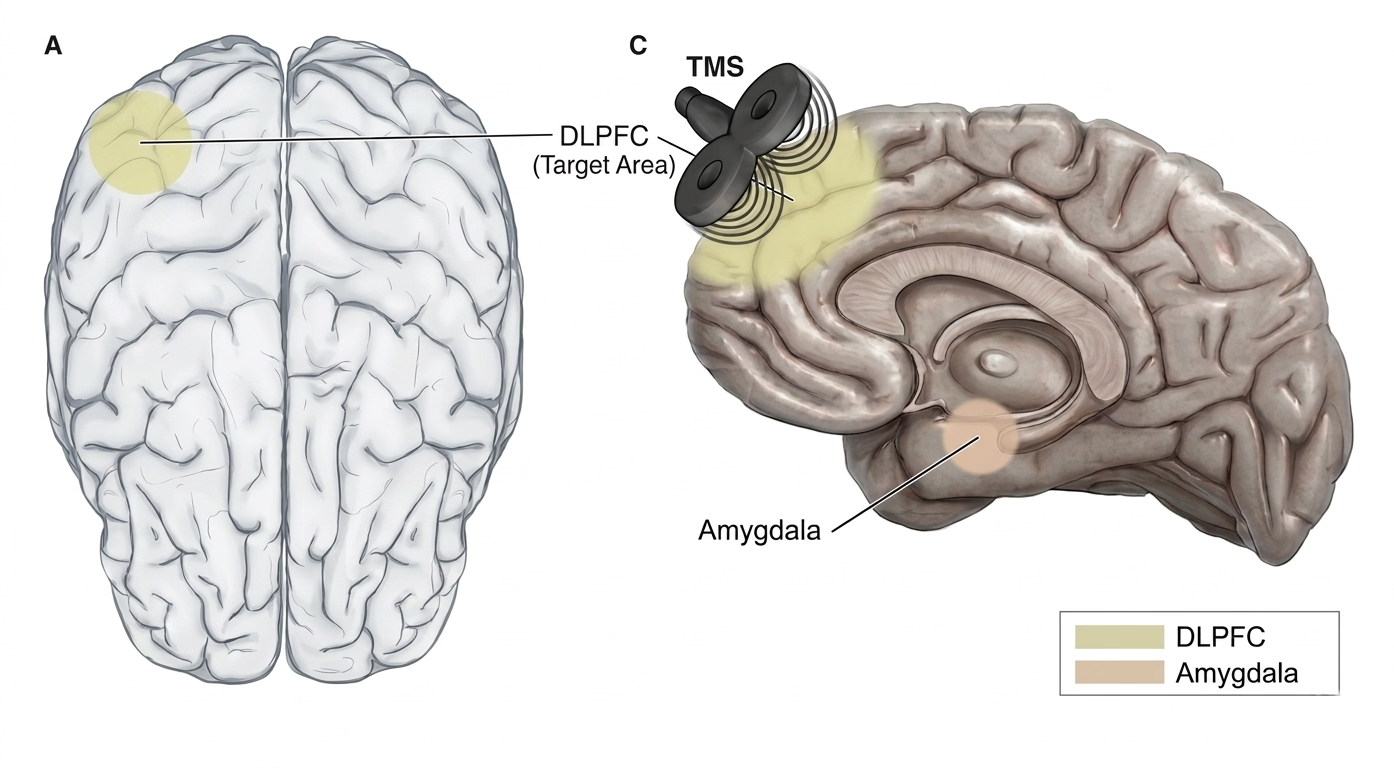
The rationale for TMS in addiction is therefore relatively intuitive: by upregulating prefrontal activity through high-frequency stimulation (typically 10 Hz, or via intermittent theta burst protocols), we can potentially strengthen the cortical circuits responsible for inhibitory control and cognitive flexibility, while indirectly modulating the hyperactive subcortical networks that drive craving and compulsive use. There is also evidence that repetitive TMS promotes dopamine release in the mesolimbic and mesocortical pathways, which may help to partially restore the blunted reward processing that characterises chronic substance use and impulsive control behaviours.
The Evidence Base: Honest and Transparent
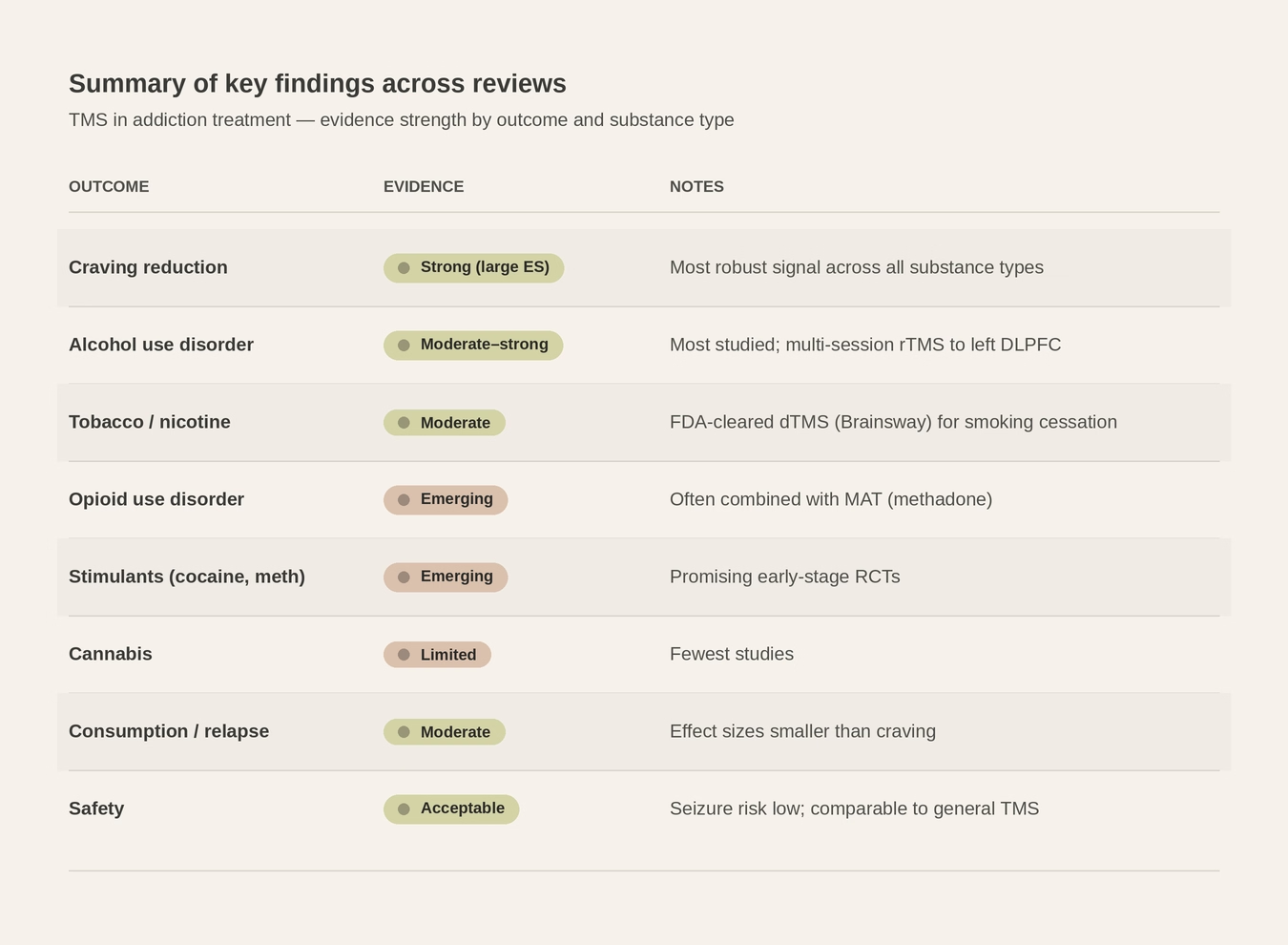
It is important to be candid about where the evidence currently stands. The body of research on TMS for substance use disorders has grown substantially, and especially in the last decade. A 2025 analysis identified 190 published articles on TMS-based addiction treatment spanning 2001 to 2023, with clinical studies representing the largest category. Systematic reviews and meta-analyses have consistently reported that repetitive TMS targeting the DLPFC produces a statistically significant reduction in craving across multiple substance types, with pooled effect sizes falling in the moderate range. Randomised controlled trials have demonstrated reductions in craving and use across tobacco, alcohol, cocaine, methamphetamine, opioid, and cannabis use disorders.
The effect size for substance use outcomes is moderate. Whilst it may not rival the magnitude of effect we see with TMS for major depressive disorder, where the treatment has a deeper and more robust evidence base, it is posited to have a moderate effect size in the context of addiction, where relapse rates with conventional treatment remain discouragingly high. It is therefore not something to dismiss. When TMS is framed as an adjunctive treatment to psychotherapy and pharmacological management, the clinical value becomes much clearer. This distinction is essential when communicating with patients, families, and referrers.
FDA-Cleared Indications: Where We Stand
The regulatory trajectory of TMS has been a slow but steady progression of approved indications.
2008
Major depressive disorder – high-frequency left DLPFC stimulation.
2013
Migraine – single-pulse TMS for acute treatment of migraine with aura.
2018
Obsessive-compulsive disorder – BrainsWay Deep TMS targeting medial prefrontal and anterior cingulate cortices.
2020
Smoking cessation – BrainsWay Deep TMS with H4 coil targeting bilateral insula and prefrontal cortices; the first FDA clearance for any TMS device in the addiction space.
The smoking cessation clearance was a landmark moment. The pivotal trial involved 262 adults with long histories of heavy smoking and repeated failed quit attempts. Among those who completed the full course, the quit rate was 28.4% in active TMS versus 11.7% in sham — a statistically significant and clinically meaningful difference. No seizures were observed; the most common side effects were headache and application site discomfort.
In parallel to the FDA developments, MagVenture TMS Therapy® received CE approval in April 2021 for the treatment of psychoactive substance use disorder (PSUD) in adults — representing the world’s first CE approval for TMS in addiction treatment. This approval, based on a naturalistic study demonstrating 69% effectiveness versus 19% for standard care, marked a significant regulatory milestone in Europe and positioned TMS as a legitimate treatment option for a broader range of substance use disorders beyond tobacco.
At present, TMS holds specific FDA clearance for nicotine addiction. This should not be confused with a lack of evidence or efficacy for other substances/addictions. The regulatory process is slow, expensive, and heavily influenced by commercial viability. The absence of a formal indication does not mean that TMS lacks utility in these contexts, it means that the pathway to formal approval has not yet been completed. In the meantime, a growing number of clinicians worldwide are delivering TMS for alcohol, stimulant, and other substance use disorders on the basis of the existing clinical literature and expert consensus.
Substance-Specific Considerations
In clinical practice, the strength of the evidence and the magnitude of benefit vary by substance. Based on the available literature and our own clinical experience, the following general patterns emerge.
Tobacco
This is where the evidence is strongest and most mature. The BrainsWay H4 coil protocol for smoking cessation is the only FDA-cleared TMS application in the addiction domain. Beyond the pivotal trial, numerous smaller studies directed at the DLPFC have shown reductions in cigarette consumption and craving.
Stimulants (Cocaine and Methamphetamine)
The data here is encouraging. One of the primary brain circuits implicated in cocaine and methamphetamine use disorders is the mesolimbic reward pathway. Both substances increase dopamine transmission throughout the mesolimbic system, which is implicated in drug-seeking and relapse.
Repeated stimulant exposure, with its associated surges in dopaminergic transmission, is thought to induce longer‑term changes in glutamatergic signalling within the prefrontal cortex, thereby exacerbating the imbalance between executive control (inhibitory) and reward networks (drug‑seeking drives). This network dysregulation is associated with impaired control, heightened cravings, and the maintenance of stimulant addiction.
Several open-label and controlled trials have shown reductions in craving and use. A large multi-site RCT (STIMULUS) should substantially clarify the efficacy of TMS for stimulant use disorders in the coming years.
Alcohol
The evidence for alcohol use disorder is moderate. Several trials have demonstrated reductions in craving with high-frequency left DLPFC stimulation, though results are somewhat inconsistent across studies, likely owing to higher heterogeneity. Emerging approaches targeting the salience network, and in particular the insular cortex, may prove more fruitful for alcohol use disorder specifically. TMS does still reduce cravings for alcohol, and in those who have an underlying depressive disorder, it may prove to be even more beneficial.
Opioids and Cannabis
The evidence base for these substances is thinner but growing. Early-stage trials suggest possible benefits, and ongoing research is exploring both conventional rTMS and theta burst protocols. These are areas to watch.
Practical Considerations
Delivering TMS within a residential rehabilitation setting has several advantages. Firstly, clients are in a structured, supervised environment. Delivering twice-daily treatment sessions is straightforward when the individual is not navigating the demands of daily life, work and triggers that drive their substance/behavioural use. TMS can be seamlessly integrated alongside psychotherapy, group work, and other therapeutic activities without disrupting the overall treatment programme.
In our clinical practice, we have found it most effective to start TMS in the second week of admission. The first week is usually focused on settling in, medical stabilisation, and managing acute withdrawal. Initiating TMS after this initial phase—when the individual is physiologically stable and more psychologically receptive — appears to optimise both engagement and tolerability.
We typically administer twice-daily sessions, five days per week, aiming for ~ 30-36 sessions. This aligns with the evidence suggesting that 30 sessions (up to 36) is likely the threshold for the maximum therapeutic benefit. Emerging accelerated protocols — notably iTBS — have compressed session times dramatically. Where a conventional 10 Hz rTMS session takes approximately 37 min, an iTBS session can be delivered in 3-4 min. This approach, pioneered in the Stanford Neuromodulation Therapy (SAINT) protocol, is now being explored for addiction applications, with early proof-of-concept studies in cocaine use disorder demonstrating both safety and tolerability.
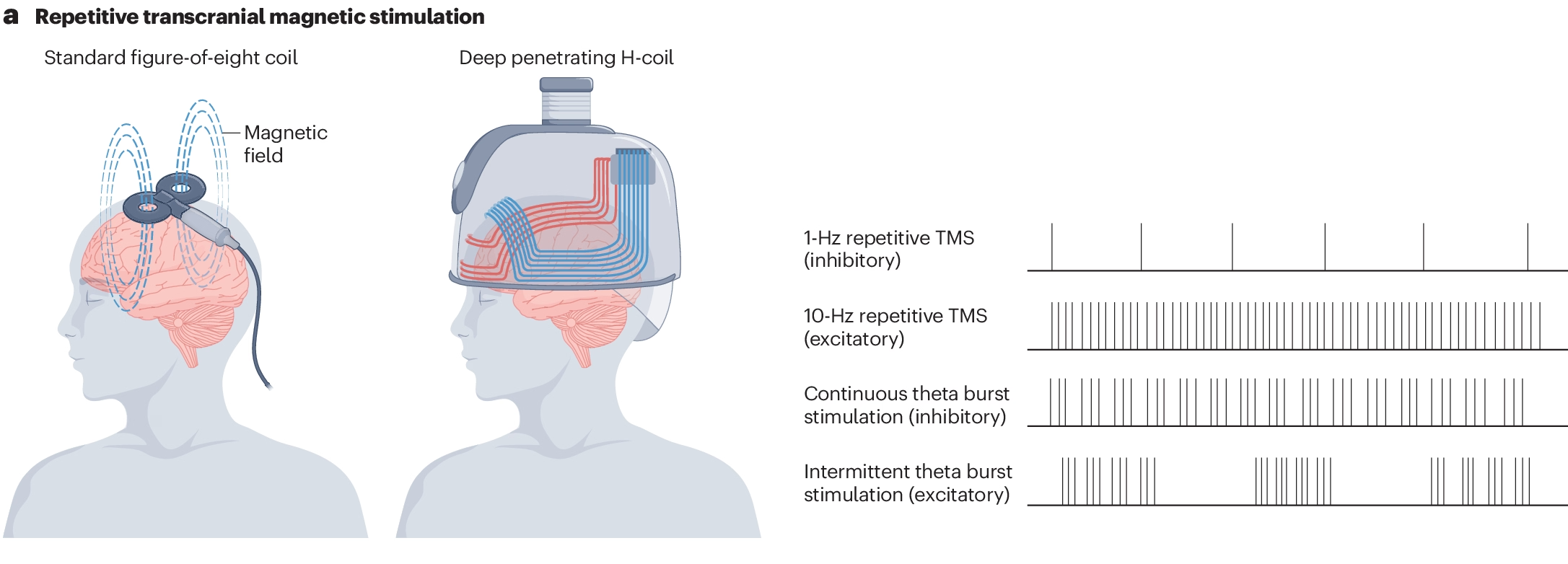
Source: Nature Reviews Psychology https://nature.com/articles/s44159-024-00291-3
Sessions are spaced 50 minutes apart, consistent with the protocols in accelerated TMS trials. This interval is thought to be necessary for the consolidation of the neuroplastic changes induced by each stimulation session.
Client Selection and Safety Screening
Not everyone entering rehabilitation is a suitable candidate for TMS, and careful screening is essential. The ideal candidate, in our experience, is someone presenting with a substance use disorder alongside a comorbid psychiatric condition such as depression, anxiety, OCD, or PTSD. For these individuals, TMS offers the possibility of addressing both the addiction and the underlying psychiatric condition simultaneously, a particularly appealing proposition given how frequently these conditions are intertwined. The individual whose depression drives compulsive substance use, or whose PTSD-related hyperarousal perpetuates reliance on alcohol or benzodiazepines to self-medicate, potentially stands to benefit the most from TMS as an adjunctive treatment.
People in the acute stages of stimulant withdrawal (particularly from high doses), those whose medications have just been significantly altered, and on medications that substantially lower the seizure threshold will generally be considered less suitable for TMS. Individuals with a pre-existing seizure disorder or significant risk factors for seizures are generally excluded. It is important to put this risk in context: large surveys suggest that seizures during TMS are rare, with rates well below 1 per 1000, when treatments are delivered within safety guidelines and obvious risk factors are excluded.
We provide all prospective clients with comprehensive information about TMS, including a summary of the research evidence, its strengths and its limitations, and a frank discussion of what they can realistically expect. TMS will be offered on an entirely optional basis, and informed consent is central to the process.
Side Effects and Tolerability
One of the most compelling features of TMS, particularly in comparison to standard drug treatments and certainly to ECT, is its favourable side-effect profile. The most commonly reported adverse effects are localised headache at the stimulation site and, in some cases, initial insomnia. Both are typically mild and self-limiting, and can be managed with standard analgesics and dose adjustment respectively. Most clients tolerate the treatment well, and dropout rates in clinical trials have generally been low.
It is worth explicitly addressing the frequent conflation of TMS with ECT, which many still make. The two treatments are fundamentally different. ECT induces a generalised seizure under general anaesthesia, with well-documented cognitive side effects. TMS does none of these things. There is no anaesthesia, no seizure, and no alteration in the level of consciousness. Clients can watch television, listen to music, or simply relax during treatment. The sensation is typically described as a light tapping on the scalp — nothing more.

Why TMS Remains Underutilised
Despite four decades of research and a steadily expanding evidence base, TMS remains markedly underutilised in addiction treatment settings worldwide. The reasons for this are multifactorial and worth examining.
First, there is the inherent conservatism of the medical profession. New treatments, even those with reasonable evidence, take time to translate to clinical practice. TMS for depression took over a decade from the initial positive trials to widespread adoption, and the trajectory for addiction applications is following a similar pattern.
Second, there are cost and infrastructure barriers. TMS machines are not inexpensive, and delivery requires trained staff, appropriate clinical space, and ongoing quality assurance.
Third, many addiction treatment services, particularly those in the public sector, are already stretched thin and may not have the capacity to introduce a new treatment modality.
Finally, there is a legitimate concern about the strength of the evidence — the effect sizes are moderate, the protocols are not yet standardised, and many of the published studies are small or methodologically heterogeneous.
These are all valid considerations. I would argue however that the evidence for TMS as an adjunctive treatment for substance use disorders is at least as strong as — and in many cases stronger than — the evidence for routine treatment as usual offered in rehabilitation settings. In a field that continues to struggle with high relapse rates despite treatment, adding a safe, well-tolerated, non-pharmacological modality seems not only reasonable but prudent.
Ongoing Treatment and Relapse Prevention
The therapeutic effects of TMS are not always immediately apparent. While some report improvements within the first ten sessions, the majority begin to notice benefits in the latter stages and, more typically, four to six weeks afterwards. This delayed onset is consistent with the neuroplastic mechanisms thought to underlie TMS’s effects and should be communicated clearly at the outset, to avoid premature disengagement due to unrealistic expectations.
For those who experience relapse following an initial successful course of TMS, maintenance or “top-up” sessions at a reduced frequency can be useful. This is analogous to the maintenance approaches for TMS for depression, where periodic booster sessions have been shown to help sustain remission. The optimal frequency and duration of maintenance TMS for addiction have not yet been formally established, but clinical experience suggests that brief courses delivered at the earliest signs of relapse or increased craving can be beneficial.
Appeal of a Non-Pharmacological Option
A subset of those presenting for addiction treatment have never been on psychiatric medication and are actively reluctant to start. For these individuals, TMS should be viewed as a particularly attractive option: a treatment that targets the neural circuitry underlying their condition without requiring them to take a daily medication.
Moving Forward
The clinical practice of neuromodulation for addiction is evolving rapidly. Several developments are likely to shape clinical practice in the coming years. Large-scale double blind RCTs like STIMULUS for stimulant use disorders (cocaine and methamphetamine) will provide the kind of robust evidence needed to move the field from promising to established. The trial is primarily a feasibility and safety test of delivering high frequency TMS in this population, but it is also powered to give early signals on abstinence and craving.
Accelerated theta burst protocols (like iTBS), may eventually compress the usual 30-session treatment course into days rather than weeks, making TMS accessible to people in short-stay or outpatient contexts.
TMS has great potential as a novel intervention for SUDs. As an adjunct offered alongside treatment as usual, it clearly represents one of the most promising additions to the addiction treatment landscape in recent years. For colleagues considering the introduction of TMS into clinical practice, I would offer this encouragement: the evidence supports its use, the safety profile is reassuring, people tolerate it well, and the potential to address both addiction and comorbid psychiatric conditions with a single modality is a distinct clinical advantage. The conservative instincts that have slowed the uptake of TMS are understandable, and are aligned with the conservative nature of medicine and psychiatry in general, and it is incumbent upon clinicians to better educate themselves on how to begin configuring, delivering and integrating TMS within existing care pathways.

Leading with Love: Starting the Conversation on Residential Treatment
Leading with Love: Starting the Conversation on Residential Treatment
By Juliana Pang

Juliana Pang
Juliana is a Registered Counsellor and Clinical Member of the Singapore Association for Counselling, with a master’s degree in counselling from Monash University. As one of The Winslow’s psychotherapists, she supports clients and their loved ones through the challenges of recovery.
There comes a time when family members realise that their loved one who has been struggling with addiction is unable to stop on their own, not even with some level of outpatient professional help. There may have been countless conversations about seeking residential treatment, but your loved one continues to refuse this option. You are feeling a sense of exasperation and powerlessness as you watch your loved one spiral towards destruction, with no clear guidance on what you could do next.
Over the course of my work with families navigating this deeply difficult situation, I have observed that there is no perfect script, no magic combination of words that guarantees the outcome one hopes for. But there are principles grounded in clinical experience and a clear understanding of how addiction works that can guide these conversations.
Understand the Disease That Has Entrapped Your Loved One
American Society of Addiction Medicine (ASAM) classifies addiction as a “treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences.”
In simple terms, addiction is not a result of a lack of willpower, nor a moral failing, nor a defiant choice. It is a mental health condition. No one sets out intentionally to become addicted to the chemicals or the behaviours.
By the time the person develops an addiction, their brain chemistry has already been significantly altered. The brain’s reward system, its memory pathways, its motivation circuits, its perception: all of these are changed in ways that make it extraordinarily difficult for the person to simply stop, even when they desperately want to. This is why you may hear your loved one promise they will quit and then not follow through.
Source: National Institute on Drug Abuse https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery
Their brains are running in a vicious loop, and they do not know how to get out of it. Further, they develop a sense of deep shame for not being able to free themselves from this mental prison, making it hard for them to receive any form of help, even when they know they need it. It is why they may lie, avoid, or act in ways that seem completely at odds with the person you know them to be.
Understanding the nature of addiction may help soften your emotions towards your loved ones and appreciate that the usual strategy of fervent reasoning or control is not going to be very effective. It does not mean we give up or be permissive, but we do have to adjust our strategies to create both emotional safety and momentum towards treatment.
Preparing Yourself for the Difficult Conversations
Before approaching your loved one for a difficult conversation, check in on your own emotional state. If you are in the grip of anger, resentment, or panic, or if your loved one is in the throes of their addiction, both parties will struggle to hear and connect with each other. Conversations tend to land better when the person initiating them is calm, clear, and coming from a place of genuine concern, and the person receiving them is momentarily free of the chemicals or the behaviours that are clouding their minds.
If more than one family member is speaking with the person affected, you would need to plan ahead on what each of you would be communicating and how this communication would be carried out. Do the work in researching treatment options and speak with relevant addiction professionals to help you craft your conversation. This would avoid overwhelming your loved one with either conflicting pieces of information or too much information. If there are family members who may not fully accept the condition of addiction or who may be emotionally triggered by the person, it may be best that they sit out the intervention conversation at this juncture. Focus on a unified approach before sitting down with your loved one for the conversation.
That said, you have to manage your expectations about the outcome of these conversations on treatment. The most well-prepared, well-timed, or the most heartfelt conversation may still not deliver the desired outcome with your loved one. It is important to recognise that one of the most powerful things you can do sometimes is to plant the seeds for change. Many people who eventually enter recovery point back to a conversation that did not seem to land at the time but stayed with them quietly, working beneath the surface and finding its way to their consciousness in rare moments of clarity.
You will likely have to deliver the intervention conversation more than once. To help you stay grounded throughout this process, you can practise emotional distancing or detachment from the expectations of outcome or any potential negative reactions to the conversations. This does not mean not caring for the person, but to create enough internal distance so that even if the conversation becomes heated, defensive, or painful, you can remain calm without taking the reactions personally. Remind yourself that you did not cause the addiction, you cannot cure it for your loved one, and you cannot control how the disease develops.
How to Approach the Conversation Itself
There is no universal script that works for every family, every relationship, every situation. But there are guiding principles that consistently make these conversations more effective.
Lead with love, and say it plainly. It may feel obvious to you that this conversation is happening because you care. But to your loved one, who is very likely carrying enormous shame and expecting judgment, it is not obvious at all. Say it directly: “I’m talking to you about this because I love you and I’m worried about you.” Say it more than once if you need to. Let it be the thread that runs through everything you do.
Use language that preserves dignity. Words matter enormously here. Avoid labels like “addict” and use “this addiction”; blame the disease, not the person. Avoid language that sounds judgemental, even if that is not your intention. Phrases like “you always,” “you never,” or “look what you have done” may feel accurate, but they activate shame, and shame is one of the most powerful drivers of continued substance use.
Avoid making the conversation about other members of the family: “Look at how you have hurt your mother” or “look at what you did to your siblings”. Instead, speak in terms of what you have observed about your loved one’s suffering and how it makes you feel. “I’ve noticed you seem to be struggling, and it worries me” lands very differently from “You have a problem and you need to fix it.”
Make room for your loved one to share their experiences. Listen more than you speak. On the surface, it may seem as if your loved one is so immersed in their addiction that nothing else seems to matter. Deep inside, they may be missing aspects of their lives that are no longer functional, hurting from lost relationships that they once treasured, grieving from the loss of their sense of self, or angry at themselves for not meeting their life’s potential.
“People struggling with addiction very often feel profoundly unheard.”
They live in a world of secrecy and isolation, and the experience of someone genuinely listening without interrupting, correcting, or steering towards a predetermined conclusion can be quietly transformative. This may be the most underrated piece of advice in the entire process.
You do not have to have all the answers at this moment. Sometimes what your loved one needs most is simply to feel that someone is willing to be present with the full, complicated truth of what they are going through. Offer unconditional presence. Let your loved one know that you will be there regardless of what happens next, whether they agree to seek help today, or whether the road ahead will have setbacks.
What to Avoid
Despite our best efforts, some of the most well-intentioned approaches can actually backfire. It is worth naming a few of them to minimise the emotional fallout.

Practising “tough love” in the form of scolding, threatening, or shaming the person almost never produces the result you are hoping for. Your loved one already feels terrible. Adding to that burden does not create motivation; it deepens the very emotional pain that drives the cycle of addiction. When a loved one is facing a health or medical crisis, it is important to still maintain a stance that balances compassion with clear, consistent boundaries. A supportive presence while upholding limits helps protect both the individual’s well-being and the relational dynamic.
Do not try to be their therapist. It is natural to want to fix things for someone you love. But addiction is a clinical condition that requires professional intervention. The most helpful thing you can do is encourage and support access to professional care. Focus your energy on what you can offer: emotional support, practical help, patience, and persistence.
If you are feeling overwhelmed and unable to hold a compassionate stance, please give yourself permission to take a step back. This does not mean that you are giving up on them; you are taking a much-needed pause so that you do not say words or do things that may hurt both of you further.
Understanding Your Treatment Options
One of the most empowering things you can do as a family member is arm yourself with knowledge about what treatment actually looks like. The landscape can feel overwhelming; there are outpatient programmes, inpatient residential programmes, therapy-based approaches, medication-assisted treatments, and various recovery support models. Terminology varies, websites are often vague, and it can be hard to know what to trust.
Our clinical team regularly navigates these complexities with families. We take a therapeutic, evidence-based approach and prioritise medical safety. You can learn more about The Winslow’s personalised residential program here.
Some Practical Steps That Can Help
Reach out to addiction treatment professionals directly. Do not rely solely on website descriptions. Call treatment centres and ask specific questions: What does a typical day of treatment look like? What therapeutic approaches do they use? What are the qualifications and experience of their clinical team? Is the facility licensed and regulated by a recognised health authority? A credible treatment provider will welcome these questions and answer them openly.
Ask about the level of care that would be appropriate for your loved one. Not everyone needs inpatient treatment, and not everyone can recover with outpatient support alone. An experienced addictions therapist can help you understand where your loved one falls on this spectrum based on the severity and duration of their addiction, their mental health, their social circumstances, and their readiness for change.
Look for experience and clinical depth. Addiction is complex and multifaceted. It frequently co-occurs with anxiety, depression, trauma, and other mental health conditions. Treatment that addresses only the surface behaviour without exploring what lies beneath it is less likely to produce lasting change. Look for programmes staffed by experienced professionals who can draw from multiple therapeutic approaches and tailor treatment to the individual.
Navigating the start of this process can feel overwhelming. Our multidisciplinary team of addiction specialists is here to provide clarity and help you determine the most appropriate next steps. If you would like to discuss your specific situation, you can schedule a confidential online consultation.
Don't Forget About Yourself
Here is something families often overlook in the urgency of helping their loved one: you need support too. Living with or caring about someone who has an addiction is emotionally draining. It reshapes your daily life, your sleep, your relationships, your sense of self. And over time, patterns develop — ways of coping, enabling, or absorbing stress — that can quietly erode your own wellbeing. It can also change the dynamics within the family system, creating secondary problems between family members, sometimes breaking families apart.
I strongly encourage family members to seek their own support, whether through individual therapy, family therapy, or support groups designed specifically for the loved ones of people in active addiction. These spaces offer something invaluable: the chance to learn, to share, and to discover things about your own patterns that you might not see on your own. Many family members who attend these groups describe moments of real revelation: realising, for instance, that behaviours they thought were helping were actually reinforcing the cycle, or that they had been neglecting their own needs for far longer than they realised.
Taking care of yourself is not selfish. It is, in fact, one of the most important things you can do for the person you are trying to help. A supported, grounded, emotionally resilient family member is a greater agent for change than one who is emotionally exhausted.
If You are Not Sure Where to Start
If all of this feels like a lot, let me simplify it.
You do not need to have the perfect conversation. You do not need to know everything about addiction or treatment before you start the conversation. You do need to show up with love, with kindness, and with the willingness to say: I see you. I am worried. I am here. And I would like to help you find support. That is enough to begin.

And if you need guidance on how to move forward, how to plan the conversation, what level of care to explore, or how to navigate the response you receive, reaching out to a professional who specialises in addiction and family support can make an enormous difference. You do not have to figure this out alone.
Recovery is possible. And it often begins not with the person who is struggling, but with the person who loves them enough to start the difficult conversation.
While this guide provides a foundation, every case is individual. To discuss your specific concerns, please contact our clinical team for a confidential discussion.